manhattan life dental claim form
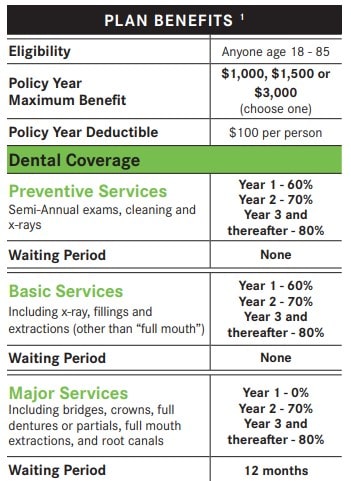
Dental Vision and Hearing insurance from ManhattanLife is designed to meet as many needs outside of standard medical insurance as possible. To process a claim please.

Manhattan Life Dental Vision And Hearing Plan Youtube
The furnishing of this form is for the convenience of the policyholder and is not an acknowledgement of liability or waiver of any right.
. Manhattan Life has been insuring Americans for over 170 years. This is a Limited Benefit Insurance Policy. Manhattan life dental claim form Monday August 8 2022 1-800-669-9030 Annuity Contract Owners.
Or contact our Customer Service department. Open the document in. VB Life Claim Form.
Affidavit of Lost Policy Form. ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care. Bank Draft Authorization Form In English en Español Beneficiary Change Form.
Annuity Cash Value and Maturity Value Request. ManhattanLife VB Claims PO Box 926169 Houston TX 77292 Customer Care. Select the form you want in our library of templates.
Duplicate Policy Request Form. Follow these simple steps to get THE MANHATTAN LIFE INSURANCE COMPANY Claim Form ready for sending. THE MANHATTAN LIFE INSURANCE COMPANY Claim Form CAUTION.
Visit the ContractPolicy Holder. It provides coverage at the dentist as well. Health Policy Cancellation Form.
Any employer group policyholder contract holder or insurer benefit plan. In the information section of the form you or your physician must fill in the following information. 247 patient benefit verification claims and remittance statements.
Submit Completed Form to. Life Health Policyholders. Affidavit of Lost Policy - International Life Policies.
As one of the. VB Cancer Claim Form Printed Name Mail to. Bank Draft Authorization Form In English.
Manhattan Life Dental Vision Hearing. For Assistance please call1-888-441-07708am - 5pm CST. Moreover to get the right results of Manhattan Life Insurance Dental Forms you need to type the correct.
Manhattan Life Dental Vision Hearing. Insureds full name and address Insureds ID Number The name and date of birth of the. Select the appropriate form category to the right.
Dental Claim Form The UFT Welfare Fund Dental Claim Form is used for two different. Select the appropriate form category to the right. To process a claim please.
The offering Companyies listed below severally or collectively as the content may require are referred to in this authorization as We or ManhattanLife Life. VB Accident Claim Form Mail to. Select the appropriate form category below.
Select the appropriate form category below. Visit the ContractPolicy Holder. You will need to know the contractpolicy.
For Assistance please call1-888-441-07708am - 5pm CST.

Western United Life Medicare Supplement Tidewater Management Group

Manhattanlife Dental Vision And Hearing Plans Are A Facebook

Manhattan Dental Youtube

Fillable Online The Manhattan Life Insurance Company Claim Form Fax Email Print Pdffiller

Manhattanlife Life Insurance Annuity And Supplemental Health Insurance

Employee Benefits Forms And Documents Risk Management Stanislaus County

Manhattanlife Client Services

Manhattanlife Manhattanlifeco Twitter

Blog Dental Vision And Hearing Insurance From Manhattanlife

Dental Vision Hearing Insurance Senior Benefit Services Inc

Manhattanlife Manhattanlifeco Twitter

Manhattanlife Manhattanlifeco Twitter

Best Medicare Supplement Plans Caring Com

Dental Vision And Hearing Insurance Senior Benefits Of Georgia
Dental Plans
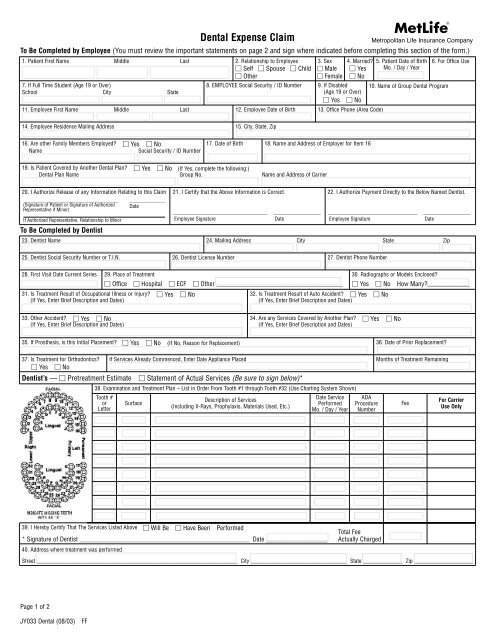
Metlife Dental Claim Form

Sammy Jaber Insurance Health Life Auto Insurance Broker

Western United Life Medicare Supplement Tidewater Management Group
![]()
Dental Vision And Hearing Insurance Dvh Manhattanlife